Death Penalty Methods & How it works

LETHAL INJECTION
The condemned person lies down on a gurney and a member of the execution team positions several heart monitors on the skin. Then, they insert a needle into usable veins, usually in the arm. There are long tubes that connect the needle through a hole in a cement block wall where there are intravenous drips. The first is a harmless saline solution that is started immediately. After that, the inmate is injected with sodium thiopental- an anesthetic, which puts the inmate to sleep. Next, pavulon or pancuronium bromide flows into the the tube, which is used to paralyze the entire muscle system and stops the inmate’s breathing. At last, potassium chloride stops the heart. Death results from anesthetic overdose and respiratory and cardiac arrest while the condemned person is unconscious. Doctors are not allowed to participate in executions. Scientists point this out as a problem, because often, injections are performed by inexperienced technicians. If a member of the execution team injected the drugs into a muscle instead of a vein, extreme pain can result.
The condemned person lies down on a gurney and a member of the execution team positions several heart monitors on the skin. Then, they insert a needle into usable veins, usually in the arm. There are long tubes that connect the needle through a hole in a cement block wall where there are intravenous drips. The first is a harmless saline solution that is started immediately. After that, the inmate is injected with sodium thiopental- an anesthetic, which puts the inmate to sleep. Next, pavulon or pancuronium bromide flows into the the tube, which is used to paralyze the entire muscle system and stops the inmate’s breathing. At last, potassium chloride stops the heart. Death results from anesthetic overdose and respiratory and cardiac arrest while the condemned person is unconscious. Doctors are not allowed to participate in executions. Scientists point this out as a problem, because often, injections are performed by inexperienced technicians. If a member of the execution team injected the drugs into a muscle instead of a vein, extreme pain can result.
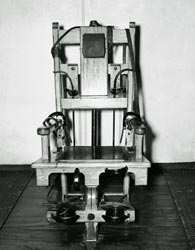
ELECTROCUTION
The person is shaved and strapped to a chair with belts that cross his chest, groin, legs, and arms. A metal skullcap-shaped electrode is attached to the scalp and forehead over a sponge moistened with saline. An additional electrode is moistened with conductive jelly and attached to a portion of the prisoner's leg that has been shaved to reduce resistance to electricity. The prisoner is then blindfolded. After the execution team has withdrawn to the observation room, the warden signals the executioner, who pulls a handle to connect the power supply. A jolt of between 500 and 2000 volts, which lasts for about 30 seconds, is given. The current surges and is then turned off, at which time the body is seen to relax. The doctors wait a few seconds for the body to cool down and then check to see if the inmate's heart is still beating. If it is, another jolt is applied. This process continues until the prisoner is dead. The prisoner's hands often grip the chair and there may be violent movement of the limbs which can result in dislocation or fractures. The tissues swell. Defecation occurs. Steam or smoke rises and there is a smell of burning.
The person is shaved and strapped to a chair with belts that cross his chest, groin, legs, and arms. A metal skullcap-shaped electrode is attached to the scalp and forehead over a sponge moistened with saline. An additional electrode is moistened with conductive jelly and attached to a portion of the prisoner's leg that has been shaved to reduce resistance to electricity. The prisoner is then blindfolded. After the execution team has withdrawn to the observation room, the warden signals the executioner, who pulls a handle to connect the power supply. A jolt of between 500 and 2000 volts, which lasts for about 30 seconds, is given. The current surges and is then turned off, at which time the body is seen to relax. The doctors wait a few seconds for the body to cool down and then check to see if the inmate's heart is still beating. If it is, another jolt is applied. This process continues until the prisoner is dead. The prisoner's hands often grip the chair and there may be violent movement of the limbs which can result in dislocation or fractures. The tissues swell. Defecation occurs. Steam or smoke rises and there is a smell of burning.

LETHAL GAS/GAS CHAMBER
the condemned person is strapped to a chair in an airtight chamber. Below the chair rests a pail of sulfuric acid. A long stethoscope is typically affixed to the inmate so that a doctor outside the chamber can pronounce death. Once everyone has left the chamber, the room is sealed. The warden then gives a signal to the executioner who flicks a lever that releases crystals of sodium cyanide into the pail. This causes a chemical reaction that releases hydrogen cyanide gas. The prisoner is instructed to breathe deeply to speed up the process. Most prisoners, however, try to hold their breath, and some struggle. The inmate does not lose consciousness immediately. According to former San Quenton, California, Penitentiary warden, Clifton Duffy, "At first there is evidence of extreme horror, pain, and strangling. The eyes pop. The skin turns purple and the victim begins to drool." (Weisberg, 1991) Caryl Chessman, before he died in California's gas chamber in 1960 told reporters that he would nod his head if it hurt. Witnesses said he nodded his head for several minutes. (Ecenbarger, 1994) According to Dr. Richard Traystman of John Hopkins University School of Medicine, "The person is unquestionably experiencing pain and extreme anxiety...The sensation is similar to the pain felt by a person during a heart attack, where essentially the heart is being deprived of oxygen." The inmate dies from hypoxia, the cutting-off of oxygen to the brain. (Weisberg, 1991) At postmortem, an exhaust fan sucks the poison air out of the chamber, and the corpse is sprayed with ammonia to neutralize any remaining traces of cyanide. About a half an hour later, oderlies enter the chamber, wearing gas masks and rubber gloves. Their training manual advises them to ruffle the victim's hair to release any trapped cyanide gas before removing the deceased. (Weisberg, 1991)
the condemned person is strapped to a chair in an airtight chamber. Below the chair rests a pail of sulfuric acid. A long stethoscope is typically affixed to the inmate so that a doctor outside the chamber can pronounce death. Once everyone has left the chamber, the room is sealed. The warden then gives a signal to the executioner who flicks a lever that releases crystals of sodium cyanide into the pail. This causes a chemical reaction that releases hydrogen cyanide gas. The prisoner is instructed to breathe deeply to speed up the process. Most prisoners, however, try to hold their breath, and some struggle. The inmate does not lose consciousness immediately. According to former San Quenton, California, Penitentiary warden, Clifton Duffy, "At first there is evidence of extreme horror, pain, and strangling. The eyes pop. The skin turns purple and the victim begins to drool." (Weisberg, 1991) Caryl Chessman, before he died in California's gas chamber in 1960 told reporters that he would nod his head if it hurt. Witnesses said he nodded his head for several minutes. (Ecenbarger, 1994) According to Dr. Richard Traystman of John Hopkins University School of Medicine, "The person is unquestionably experiencing pain and extreme anxiety...The sensation is similar to the pain felt by a person during a heart attack, where essentially the heart is being deprived of oxygen." The inmate dies from hypoxia, the cutting-off of oxygen to the brain. (Weisberg, 1991) At postmortem, an exhaust fan sucks the poison air out of the chamber, and the corpse is sprayed with ammonia to neutralize any remaining traces of cyanide. About a half an hour later, oderlies enter the chamber, wearing gas masks and rubber gloves. Their training manual advises them to ruffle the victim's hair to release any trapped cyanide gas before removing the deceased. (Weisberg, 1991)

HANGING
the inmate may be weighed the day before the execution, and a rehearsal is done using a sandbag of the same weight as the prisoner. This is to determine the length of 'drop' necessary to ensure a quick death. If the rope is too long, the inmate could be decapitated, and if it is too short, the strangulation could take as long as 45 minutes. The rope, which should be 3/4-inch to 1 1/4-inch in diameter, must be boiled and stretched to eliminate spring or coiling. The knot should be lubricated with wax or soap "to ensure a smooth sliding action," according to the 1969 U.S. Army manual. (The Corrections Professional, 1996 and Hillman, 1992)
Immediately before the execution, the prisoner's hands and legs are secured, he or she is blindfolded, and the noose is placed around the neck, with the knot behind the left ear. The execution takes place when a trap-door is opened and the prisoner falls through. The prisoner's weight should cause a rapid fracture-dislocation of the neck. However, instantaneous death rarely occurs. (Weisberg, 1991)
If the inmate has strong neck muscles, is very light, if the 'drop' is too short, or the noose has been wrongly positioned, the fracture-dislocation is not rapid and death results from slow asphyxiation. If this occurs the face becomes engorged, the tongue protrudes, the eyes pop, the body defecates, and violent movements of the limbs occur. (The Corrections Professional, 1996 and Weisberg, 1991)
the inmate may be weighed the day before the execution, and a rehearsal is done using a sandbag of the same weight as the prisoner. This is to determine the length of 'drop' necessary to ensure a quick death. If the rope is too long, the inmate could be decapitated, and if it is too short, the strangulation could take as long as 45 minutes. The rope, which should be 3/4-inch to 1 1/4-inch in diameter, must be boiled and stretched to eliminate spring or coiling. The knot should be lubricated with wax or soap "to ensure a smooth sliding action," according to the 1969 U.S. Army manual. (The Corrections Professional, 1996 and Hillman, 1992)
Immediately before the execution, the prisoner's hands and legs are secured, he or she is blindfolded, and the noose is placed around the neck, with the knot behind the left ear. The execution takes place when a trap-door is opened and the prisoner falls through. The prisoner's weight should cause a rapid fracture-dislocation of the neck. However, instantaneous death rarely occurs. (Weisberg, 1991)
If the inmate has strong neck muscles, is very light, if the 'drop' is too short, or the noose has been wrongly positioned, the fracture-dislocation is not rapid and death results from slow asphyxiation. If this occurs the face becomes engorged, the tongue protrudes, the eyes pop, the body defecates, and violent movements of the limbs occur. (The Corrections Professional, 1996 and Weisberg, 1991)
